
Healthcare M&A: strategies for successful infrastructure integration
Recent Articles
Healthcare M&A: strategies for successful infrastructure integration
Infrastructure integration planning sometimes slips through the cracks during a healthcare merger or acquisition. Here’s how to do it right.

The United States healthcare system is undergoing many transformative changes, and among them is a growth in consolidation. According to a September 2021 report by Fierce Healthcare, there had been 187 Mergers and Acquisitions to date in 2021 – nearly double what it was for the same period the previous year. Smaller hospitals, especially those located in rural areas, are being integrated by larger healthcare systems at a rapid pace.
Healthcare mergers can make sense for many reasons. For one, the smaller hospitals gain the ability to attract customers by leveraging the brand visibility of a well-known health system. The deep pockets of a large system also help smaller hospitals complete infrastructure improvements, upgrade equipment and recruit better-trained physicians. Ultimately, this benefits the patients, as the rural facilities can provide quality care closer to home, and patients no longer have to travel long distances to get the treatment they need. The primary healthcare system benefits from the increase in market share.
Why do healthcare integration efforts fail?
Successful execution of a healthcare merger or acquisition can be quite challenging. The changes resulting from M&A can induce quite a bit of uncertainty, disorientation, and navigational challenge, both for the patient and the target healthcare system. This adds stress and anxiety to the patient experience, which is often directed towards the clinical staff, thereby increasing the risk of medical errors and lowering patient satisfaction scores.
The facility is an important factor that ties staff, patient satisfaction and revenue streams together. But too often, Infrastructure Integration planning sometimes slips through the initial financial and legal modalities of an M&A strategy session. To counter that, executives should plan for infrastructure integration during the visioning stages of M&A. For an Infrastructure integration strategy to be successful, planning, market analysis, feasibility studies and facility condition assessments are needed. Needs assessment reports and customer satisfaction surveys can also provide valuable insights into the strategy and goals.

What makes facility integration successful?
Ultimately, the goal of integration is to improve patient care, which involves a dynamic process of optimization leading towards patient satisfaction. Two of the most successful means of such optimization are space standardization and space flexibility.
Standardization simplifies processes, tasks, and designs. It facilitates the process of reusing facilities, enhances patient safety, reduces staff error and helps organize patients’ activities. One of the prerequisites of successful standardization is stakeholder engagement to choose healthcare products and services. Simply put, a product or service is a good choice if it is recommended by its key beneficiaries. To gather this feedback, the process should involve healthcare administrators, caregivers, former patients and family members sharing their experience and insights. From an M&A perspective, this is important to make sure the standardization and facility integration goals suit the culture and people of the region.
Stakeholder engagement, feedback and buy-in give healthcare systems evidence-based goals that ensure quality patient care while supporting fiscal responsibility. With solid goals in place, and with leadership commitment, standardized guidelines give healthcare administrators evidence-based basis to sell their groundbreaking ideas, implement new processes and continuously improve.
Standardizing spaces
The more the processes and designs are standardized, the easier and more efficient the staff will find it to adapt and function in that environment. For example, in a standardized patient room, the staff always knows where to find equipment and supplies. Staff can address the patient in a routine manner and make observations/assessments in the same order. Checking and administering medications occur in the same pattern for every patient, and documentation of patient care occurs in the same system in the same location in each room. This leads to fewer medical errors and substantially reduces wasted time.



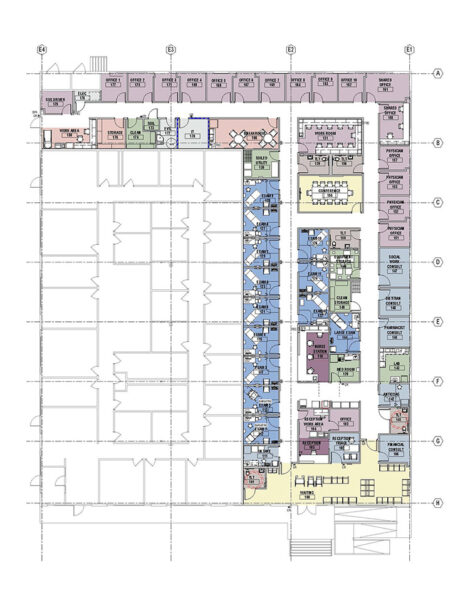
Flip through the slider above to get a picture of a standardized clinic design.
This is also true of standardized floor plans for patient care units. Administrative areas, decentralized clinical work areas, imaging viewing areas, meeting rooms, offices, supply and equipment storage areas, clean and soiled utility and housekeeping rooms should all be placed in the same location on all floors. This standardized design makes it easier and more efficient for physicians and staff to move about in the facility. Supply and dietary staff who deliver goods to each unit can do their job more efficiently in a standardized environment. Further, standardization can reduce the cost of the design process and make for easier future expansion or addition of services.
Making spaces more flexible
According to a 2004 study in the American Journal of Critical Care, each time a patient is transferred from one unit to another, their length of stay is increased by approximately half a day. In addition, transferring a patient increases the opportunity to lose patient items, creates a potential for a staff injury from pushing a heavy bed, decreases patient and family satisfaction, and creates delays in treatment until other staff catch up with the patient in a new location.
Flexibility improves productivity and saves time by allowing different functions to take place within an intelligent, multi-purpose space. The use of common spaces for multiple-purpose functions reduces staff and patient travelling distance and mitigates the pressure associated with transferring fragile patients from one functional space to the next for treatment.

Another flexibility strategy is the use of standardized patient rooms. This approach, also known as the “universal” or “acuity-adaptable” room, allows facilities to swing beds between specialties based on patient demographics. In facilities that do this well, patients can remain in their rooms for the duration of their stays while staffing levels flex according to the patient’s acuity (acuity flexible staffing).
According to the book Evidence-Based Design for Healthcare Facilities by Cynthia McCullough, specialty medical services such as cardiac, trauma or burn work well with an acuity-adaptable model of care. However, some who have changed to this model find it challenging to implement and keep up with the caregiving requirements, primarily because of staffing competencies. However, the acuity-adaptable room has many benefits for the patient. Depending on circumstances, nursing leadership should at least consider a staffing pattern that allows staff to flex according to acuity while the patient remains in the same room.
Administrators must always be willing to push for a baseline standardization in the patient environment to ensure it can support many models of care. With a balanced emphasis on serving both the patient and the staff’s needs simultaneously, these initiatives can have significant impacts on infrastructure flexibility.
How can healthcare systems prepare to standardize?
Healthcare systems looking at a merger or acquisition should form an internal team tasked with procuring and processing inputs from various stakeholders into a well-developed set of standards tailored to the organization. This team should include a network of architects, planners, vendors, and manufacturers who will support the installation of standard conditions. Begin the process by designating pilot projects, for example: patient rooms, exam rooms or nurses’ stations.
It is important to note that standardization, while effective in providing structured methods, is still a guideline and not a one-size-fits-all solution. Some locations may need to adapt alternate options that account for different geographical and demographic conditions. This added layer of flexibility empowers healthcare providers to meet the diverse cultural and healthcare needs of the demographics they serve and further supports their vision of continuous improvement to optimize conditions and quality of care.
How can LEO A DALY help?
LEO A DALY has contributed to positive outcomes of major capital asset planning initiatives for more than 100 years. During a typical project visioning session of standardization, we do not limit the key stakeholders to facilities personnel only; but also include various groups such as nurse managers, patient experience specialists, executive leadership, and community members like former patients and their families. The more exhaustive the feedback, the better informed decisionmakers can be in their development of standardization guidelines.
We’ve led numerous infrastructure improvement and integration efforts with multiple healthcare organizations and developed standards for many of our clients across the country, including a major revision to the VA Design Guide in 2020. As a team, we have consistently proven our expertise and added value to develop standards for healthcare facilities integration.
White paper: Catalytic typologies
White paper: Catalytic typologies
Rethinking latent urban and suburban spaces for post-pandemic recovery

COVID-19 has had widespread impacts on the commercial real estate industry, reducing cash flow and slowing new investment in hotel, retail, office, co-working and co-living. As the pandemic continues, large cities have seen a collapse in the activities that make urban life economically and socially vibrant. While the magnitude of the pandemic’s long-term effects on cities remain to be seen, it is clear the way urban dwellers live, work, buy, sell, socialize and travel will be altered for many years to come.
This white paper by Global Design Principal Irena Savakova, Design Director Daniel Yudchitz, Chief Sustainability Officer Ellen Mitchell-Kozack and Director of Planning and Urban Design Chia-Lung Chang examines latent urban and suburban spaces in search of opportunities to catalyze economic recovery. Under the umbrella of “catalytic typologies,” we present a mix of concept studies that apply wellness-focused planning and architecture strategies to add value and vibrancy.
About the authors
 Irena G. Savakova, RIBA, LEED AP BD+C, is an award-winning architectural designer with 25 years of experience developing projects for federal, commercial and educational facilities in the U.S. and internationally. She enjoys an industry-wide reputation for her creativity, passion and knowledge in managing complex core and shell developments, interiors and space-planning projects. Irena began her design career in Bulgaria. In 1991, she graduated with a Master of Architecture degree and began practicing in the European Union, where she is licensed as a registered architect. In 1995, she earned a Master of Architecture degree from the University of Maryland at College Park.
Irena G. Savakova, RIBA, LEED AP BD+C, is an award-winning architectural designer with 25 years of experience developing projects for federal, commercial and educational facilities in the U.S. and internationally. She enjoys an industry-wide reputation for her creativity, passion and knowledge in managing complex core and shell developments, interiors and space-planning projects. Irena began her design career in Bulgaria. In 1991, she graduated with a Master of Architecture degree and began practicing in the European Union, where she is licensed as a registered architect. In 1995, she earned a Master of Architecture degree from the University of Maryland at College Park.
 Daniel Yudchitz, AIA, NCARB, LEED AP, grew up as the son of an architect, which undoubtedly instilled a passion to create and explore the built environment in Daniel. He believes architecture is about allocating resources strategically to achieve maximum impact, which requires meaningful architectural expression within constraints of time and money. The challenge is in the discovery of opportunities for design impact that transcend those limitations. Daniel focuses on creating strategies for aspirational design expressions to reinforce the client’s mission and enhance building functionality in a sustainable, economical and impactful manner.
Daniel Yudchitz, AIA, NCARB, LEED AP, grew up as the son of an architect, which undoubtedly instilled a passion to create and explore the built environment in Daniel. He believes architecture is about allocating resources strategically to achieve maximum impact, which requires meaningful architectural expression within constraints of time and money. The challenge is in the discovery of opportunities for design impact that transcend those limitations. Daniel focuses on creating strategies for aspirational design expressions to reinforce the client’s mission and enhance building functionality in a sustainable, economical and impactful manner.

Ellen Mitchell-Kozack, AIA, LEED BD+C, WELL AP, SEED, leverages LEO A DALY’s integrated design expertise to affect positive change. She applies a humanitarian and environmental lens to architecture to benefit clients, the communities we live in and the future of our planet. As chief sustainability officer, Ellen leads the firm’s strategic initiatives in sustainable design worldwide, including Environmental Social & Governance, alignment with the UN Global Compact and Sustainable Development Goals, carbon footprint assessment and social impact.
 Chia-Lung Chang, AIA, works closely with executive and studio leadership to develop and execute strategic direction for the firm’s global planning and urban design practice. An award-winning planner and architect, he is widely recognized for the forward-looking leadership he brings to his work and regularly lectures on smart cities, quality of life and long-term sustainability in the built environment. Chia is also an expert at managing and designing complex projects that require big picture, resource-driven solutions. His planning and urban design portfolio encompasses work across the globe.
Chia-Lung Chang, AIA, works closely with executive and studio leadership to develop and execute strategic direction for the firm’s global planning and urban design practice. An award-winning planner and architect, he is widely recognized for the forward-looking leadership he brings to his work and regularly lectures on smart cities, quality of life and long-term sustainability in the built environment. Chia is also an expert at managing and designing complex projects that require big picture, resource-driven solutions. His planning and urban design portfolio encompasses work across the globe.
Space optimization through relocation
Recent Articles
Space optimization through relocation
LEO A DALY’s diverse and creative teams combine planning, architecture, engineering and interiors expertise to offer a holistic response to our clients’ challenges. With this broad view of a project from beginning to end, and involvement in every step of the way, we know that planning is a vital component in a successful project. Our healthcare team knows the path to a successful project at completion, begins at inception. In our Dallas studio, the healthcare team strives to plan medical spaces that allow healthcare systems to provide uncompromised care and transform the patient and caregiver experience through design.


As part of preparations to sell the Old Parkland Hospital Campus, our team was commissioned to help facilitate the move of eleven departments, clinics, and community outreach programs into six different buildings. After project kick-off, the team toured and analyzed each department in their existing spaces to gain an understanding of their processes, flows, and needs as they relocated into a new space. Many of the departments were feeling cramped since their services, client and patient population, and community service programs had grown since first occupying their current spaces. Through user interviews, information gained from the tours, and the existing floor plans, the team formulated new space programs. These new programs demonstrated that most of the eleven departments required more square footage than their current space. However, each department was limited to a new footprint equal to their current square footage. This limitation gave us the opportunity to maximize efficiencies and streamline floor plans in the new locations to give Parkland areas that truly improved their ability to work and serve the Dallas community.
Providing Parkland with a realistic program for new spaces allowed them to vet nearby leasable locations as well as available space within the new hospital. As the LEO A DALY and Parkland teams worked together through scheduling and logistics of the relocations, the requirement for several short-term enabling moves were identified. Using the developed program, our team was able to quickly pivot and assist Parkland with identifying vacant spaces within their campus that could accommodate these departments using existing room layouts and making minimal modifications. This enabled the departments to relocate quickly but still operate effectively in their interim locations. When complications arise on complex projects, a nimble, creative, and collaborative team ready to roll up their sleeves to provide new solutions can be the difference between a project completely halting and one that continues.
Though all eleven departments are a part of Parkland, each is also an individual client with their own unique processes and needs – this was certainly not a case of one solution fits all. LEO A DALY incorporated feedback from patient round table discussions and hosted multiple design meetings with each department, inviting representatives from all levels, from receptionist through care providers, to ensure the new design would accommodate the needs of everyone.
During planning and design of the Geriatrics Clinic, ongoing discussions revolved around the design, layout, and equipment configuration of the exam room. The team determined a full-scale mock-up of the exam room would be more beneficial than 2D or 3D drawings. In a mock-up, users experience the space as it would exist in its final state and are to make modifications and adjustments – from small changes such as moving an outlet six inches to larger modifications such as moving a sink or door. Without the mock-up, the functionality of the space isn’t realized until well into construction, at which point modifications would impact both budget and schedule. Our team has employed mock-ups in a variety of projects and sizes, from individual rooms to whole departments, to help our clients make the right operational decisions at the right time.



Planning projects within limited space is an exercise in give and take, requiring care and thought while helping clients navigate prioritizing needs and minimizing excess. One example would be a client’s decision to incorporate six-foot-wide patient corridors in a clinic early in planning due to a high level of wheelchair and mobility impaired circulation. Prioritizing this decision early allowed us to thoughtfully and proactively plan the clinic to accommodate wider than required corridors and deliver a functional department layout instead of a reactionary design.


Setting a project up for success starts on day one before the team hits the drawing board. My team finds success when, in partnership with the client, we:
- Set goals early and for all aspects of the project
- Revisit project and client goals periodically and evaluate the current design against them to ensure the project is progressing towards them.
- Gain an understanding of the functional and operational needs of the space
- Invite the right people to the table to deliver a solution that considers all users
- Identify necessities and wish list items in order to prioritize program and design elements
Our world is always changing, from building and health codes to unprecedented events like pandemics. Our team looks at each design challenge from multiple perspectives and strives to stay up to date on best practices, incorporating our expertise to provide the best individualized solutions for our clients. We understand every decision has an impact on the schedule, budget, care provider, and patient experience. We want to help you provide the best care and better serve your community.
 About the author
About the author
About the author 
Rebecca Davis focuses on creating healthcare spaces with holistic experiences to enrich the patient experience. During her 20 years of practice, Rebecca has been dedicated to the planning, design and management of healthcare projects, with a passion and expertise in behavioral health spaces, oncology and support services departments, such as labs and pharmacies. Her portfolio includes more than 6 million SF of facilities, from small renovations and community hospitals to specialty medical centers and research facilities.
David City Downtown Revitalization and Infrastructure Improvements
David City Downtown Revitalization and Infrastructure Improvements
David City wanted to improve the quality of life for its citizens and the experience for visitors. This $9.6 million project revitalized critical infrastructure and transformed downtown into a destination for people passing through. LEO A DALY designed all improvements, led stakeholder outreach and assisted the city with the funding process throughout the project. We also helped the city obtain $1.8 million in funding from Nebraska Department of Transportation for roadway and storm-sewer upgrades on Highway 15.
Following approval of our concept plan, we were selected to work directly with the city council and stakeholders of David City and Butler County to design the infrastructure upgrades for revitalization over an eight-block area within the downtown core. Our work with Butler County led to an additional $200,000 to upgrade infrastructure around the county courthouse in David City.
Working with David City staff, we developed a revitalization plan. Among other objectives, we aimed to improve the aging water system, which required street replacement. The existing streets were wide, with parking on both sides and in the middle of the street. Before finalizing a plan, we sought public input to identify the vision of downtown business owners and citizens of David City.
We held three daylong technical sessions at the public library. They were open to the public. Additionally, we conducted one-on-one visits to downtown businesses. We also distributed a questionnaire with monthly utility bills. More than 30 percent of residents responded. We analyzed all input and developed a final plan for eight blocks within the core of the city. Our plan was approved by the David City Planning Commission and City Council. It addressed aging water lines and the storm sewer system, crumbling sidewalks, lack of ADA compliance and exhausted road surfaces.
Implementation phase considerations included:
• Use of aerial photography to collect topographic information
• Tunnel walks to determine location, depth, and width of tunnels for demolition
• Meetings with landowners to discuss closure of tunnel access and coal chute demolition
• Public progress meetings
• Bidding and negotiation for contractor selection
• Construction administration
Ongoing cost control of the $9.6 million project was critical. We worked closely with city council to monitor the project’s cost, and we assisted with critical decisions that might impact it. Our design team kept David City residents and business owners aware of all construction activities with a bi-weekly newsletter for the duration of the project.
Client
At a glance
Design of 15 blocks through downtown and intersecting streets, including sidewalk updates, a new storm sewer system and a new electrical system that serves new energy-efficient street lights.
Features
Enhanced walkability and accessibility
New utility and roadway infrastructure
Services
Planning
Civil design
Electrical engineering
Funding assistance
Bidding procurement and oversight
Construction administration
Construction observation

Video: Planning for a resilient post-COVID environment
Video: Planning for a resilient post-COVID environment
Planning and sustainability leaders discuss impact of health crisis on the design of the built environment
Commercial Market Sector Leader Kristina Crawley sat down with two LEO A DALY experts whose practices directly influence commercial placemaking and real estate development, Chia-Lung Chang, Director of Planning and Urban Design, and Ellen Mitchell-Kozack, Chief Sustainability Officer, to discuss the impact of the coronavirus pandemic on future commercial design considerations.
Listen to their discussion surrounding the long-term effects of a worldwide health crisis on the understanding and design of the built environment in this roundtable video.
Chris M. Rupert

With more than 15 years of experience planning and designing projects for healthcare, education and government, Chris has helped many of our clients realize their project visions. She has planned projects of all sizes, including medical clinics, libraries and law-enforcement complexes. She frequently works with regional and federal agencies, national guard units and universities, and her work includes the Lied Scottsbluff Public Library Addition and Renovation.
From small feasibility studies to complete master plans for 10,000+ acres, Chris enjoys the process of drawing out a client’s vision for the future and collaborating to create a roadmap to make their vision a reality. She brings an inquisitive approach to every interaction, as well as good humor and her signature laugh.
Irena G. Savakova

Irena is an award-winning architectural designer with 25 years of experience developing projects for federal, commercial and educational facilities in the U.S. and internationally. She enjoys an industry-wide reputation for her creativity, passion and knowledge in managing complex core and shell developments, interiors and space-planning projects.
Over the decade, Irena has led or contributed to the architectural design of new signature facilities for the U.S. Department of State, Social Security Administration, National Guard Bureau, Air National Guard, Naval Facilities Engineering Command and NASA.
Irena began her design career in Bulgaria. In 1991 she graduated with a Master of Architecture degree and began practicing in the European Union, where she is licensed as a registered architect. In 1995, she earned a Master of Architecture degree from the University of Maryland at College Park.